
Path: Product, Probability, PRO, Price...
Path dependence and planning

The molecule that goes into the clinic and the molecule that you launch are the same. The only thing that separates them is what you learn. What you learn, however, is inevitably constrained by your choice of path.
The molecule is not your product. That product is a product of a thousand decisions: not just indication or positioning within indication, but dose, device, diagnostic, and a lot more.
Each of those decisions affects your probability of success - technical success, regulatory success and commercial success. Those probabilities are held in tension with each other: optimising for one often negatively affects at least one of the others, like squeezing a balloon. The worst approach to this is the one that a linear process forces: fix one and hope to massage the others. In the traditional pharma approach, someone already has their foot on part of the balloon.
Once someone (else) makes a decision on path, your room to optimise your own probability is limited. This path dependence limits any mathematics you can bring to bear on cost-effectiveness analysis. Making the case for the value of your drug (see Peter Kolchinsky’s passionate defence of value…) is less ‘of all the ways in which we could deliver value to patients, this represents the peak’ than ‘of all the ways that we were left with, this is the best story…’
The definition from economics works for pharma decisions too:
Path dependence is when the decisions presented to people are dependent on previous decisions or experiences made in the past.[1]
Path dependence exists when a feature of the economy (institution, technical standard, pattern of economic development etc.) is not based on current conditions, but rather has been formed by a sequence of past actions each leading to a distinct outcome.[2]
So far, so mathematical… However, if we’re to pretend we’re patient-focused, or patient-centric, or patient-infused, then we need to accept that the ‘patient-relevant outcomes’ (my preferred version of PRO), or even the traditional PROs, are working within limited guardrails, once they’re applied downstream. If you want to optimise them, you’d have to go back in time, swim back upstream, to an earlier decision.
I’ll repeat my earlier cartoon, which illustrates path dependence:
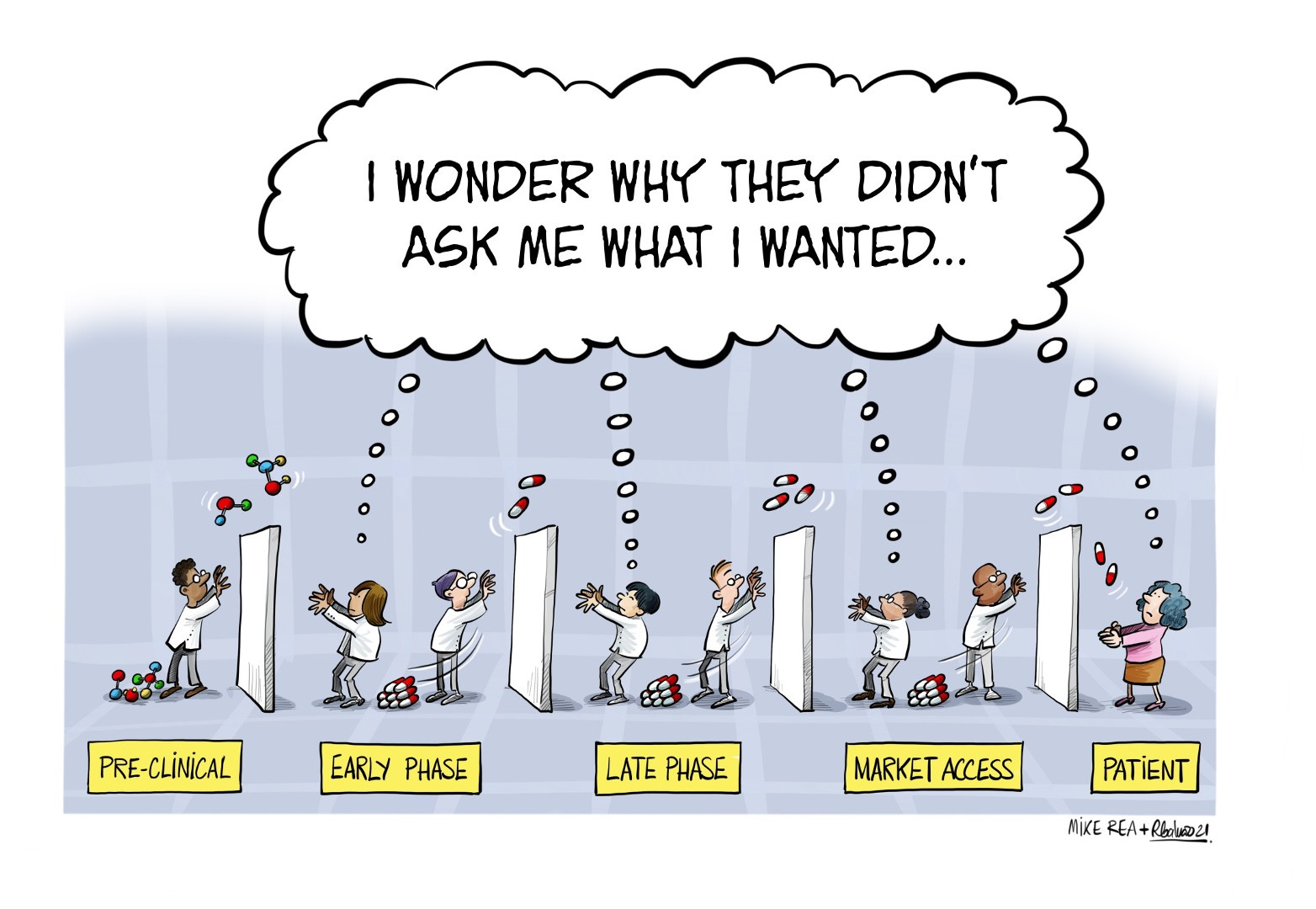
The only solution to this constraint is that paths are chosen with all of the probabilities in mind. However, in early phase, the confidence intervals on those probabilities are too wide to be relied upon. Instead, an approach that holds open optionality until those uncertainties can be reduced is both cost-effective (fewer barren paths that lead to dead ends) and valuable to patients whose unmet needs can be considered, and planned into development. That approach is a Learning approach. Doing it better than your competition is where the Asymmetry matters…