
You Keep Using That Word
Innovation Theatre in Pharma (15 Years Later)

I used this exact image about 15 years ago. Not sure pharma has got better in general. (I’ve failed 😅)
You keep using that word. Innovation.
I do not think it means what pharma think it means.
Fifteen years on, and the line still lands like a punch in the gut every time I see another press release crowning some incremental tweak or shiny pilot as “transformative innovation.”
The Gap Between Word and Reality
In pharma, we love the word innovation. We hate what it actually demands.
Invention is coming up with something new - a molecule, a target, a platform, a clever bit of tech. Innovation is turning that invention into something that creates real, sustained value for patients and the business. As I’ve said many times: invention is necessary but not sufficient.
Most of what gets labelled “innovation” sits firmly in the invention bucket - or worse, in the pure marketing bucket. A new formulation. A digital app that patients download twice. An AI pilot that generates pretty graphs but never touches a clinical trial. A gleaming innovation lab with bean bags and whiteboards that hosts impressive demos but ships nothing to market.
This is what people now call innovation theatre. (Well, Steve Blank was the person who (I think) first used it, so it’s good that ‘people’ have caught up…)
What Innovation Theatre Looks Like
Innovation theatre is the corporate equivalent of a Hollywood set: impressive from the front, completely hollow when you walk around the back.
You’ve probably seen it (or run it):
Hackathons and idea challenges that generate thousands of Post-its and zero implemented solutions.
Innovation labs and accelerators that partner with flashy startups, announce grand collaborations, and quietly sunset the projects two years later.
Chief Innovation Officers who’ve become professional AI PowerPointers.
AI/digital health initiatives that move from hype to inspection-grade reality far slower than promised.
These activities create activity. They create great photos for the annual report. What they rarely create is new revenue from new drugs or meaningfully better patient outcomes at scale.
What the 2026 Pharmaceutical Innovation + Invention Index Reveals
This year marks the 15th anniversary of the Pharmaceutical Innovation + Invention Index - the longest-running benchmark of its kind. I invented/ created the index after asking myself (and anyone I could bore…) the same provocative question: if you gave the same molecule to two different companies in early phase, who would be more successful and why? No-one then, and I assume no-one now, believed the answer was ‘yes’ but pharma still, 15 years later, acts as though it definitely is.
The 2026 results are clear.
Innovation and invention converge at the top. Eli Lilly and Company is #1 on both the Innovation Index (commercial return from invention) and the Invention Index (pipeline novelty) for the first time. Its incretin platform - anchored in Mounjaro/Zepbound and extended through retatrutide, orforglipron, and more - shows exactly what real innovation looks like: platform science paired with disciplined late-stage execution and commercial delivery.
Sanofi climbed +19 places to #3 on the Innovation Index - the biggest jump in the Top 10 - by becoming a launch- and readout-driven organization. GSK rose +10 places by translating a strategic shift into oncology, respiratory, and vaccine wins. These companies aren’t just inventing; they’re refreshing their portfolios with meaningful revenue from recent launches (the Freshness Index is revealing, alongside the Fragility Index - which shows who’s exposed to gaps).
By contrast, Bristol Myers Squibb dropped 14 places on the Innovation Index despite continued research output. The reason? A concentration of Phase 3 setbacks and loss-of-exclusivity pressure. Scientific activity without sustained late-stage delivery gets penalised. That’s the index calling out innovation theatre in real time.
Why Innovation Theatre Persists
Because it’s easier.
Real innovation is messy, risky, and slow. It requires killing sacred cows, reallocating real budget, accepting public failure, and having hard conversations with regulators, payers, and internal stakeholders. The fact that revenue (or the inverse, not losing invested dollars that don’t repay) shows up 10-15 years after those decisions - a very delayed response - makes it hard to show that you just made the right decision.
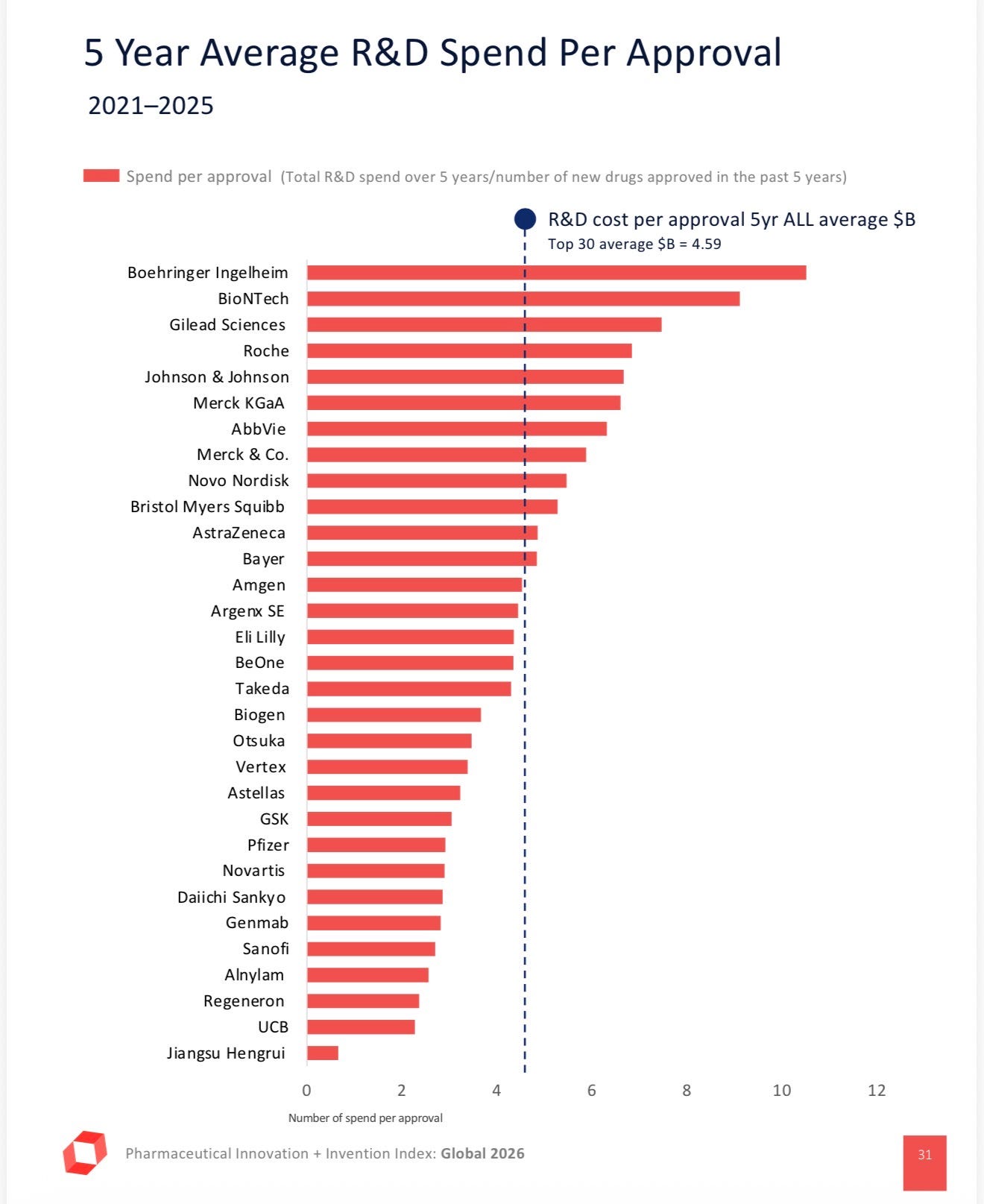
The effects show up in charts like this (downloadable from IDEA’s website). Imagine still believing or using ‘average’ costs per launch in your eNPV…
Innovation theatre lets you signal clever stuff, scientific stuff, to investors, recruits, and the board without making those tough choices.
What Real Innovation Actually Requires
Real innovation looks less glamorous and more like hard work:
Building repeatable systems around inventions (the “garage” that actually commercializes the playground ideas).
Ruthless prioritization - saying no to 99% of things so the 1% can succeed.
Measuring what matters: not activity metrics, but Freshness (percentage of revenue from recent launches) and real health-economic impact.
Accepting asymmetry - some bets will be huge winners, most will fail, and that’s the only way the maths works. Placing lots of bets, and learning from small bets quickly, helps here.
The companies that top the indices consistently do more of the latter and less of the former. They treat innovation as a discipline, not an event or a department.
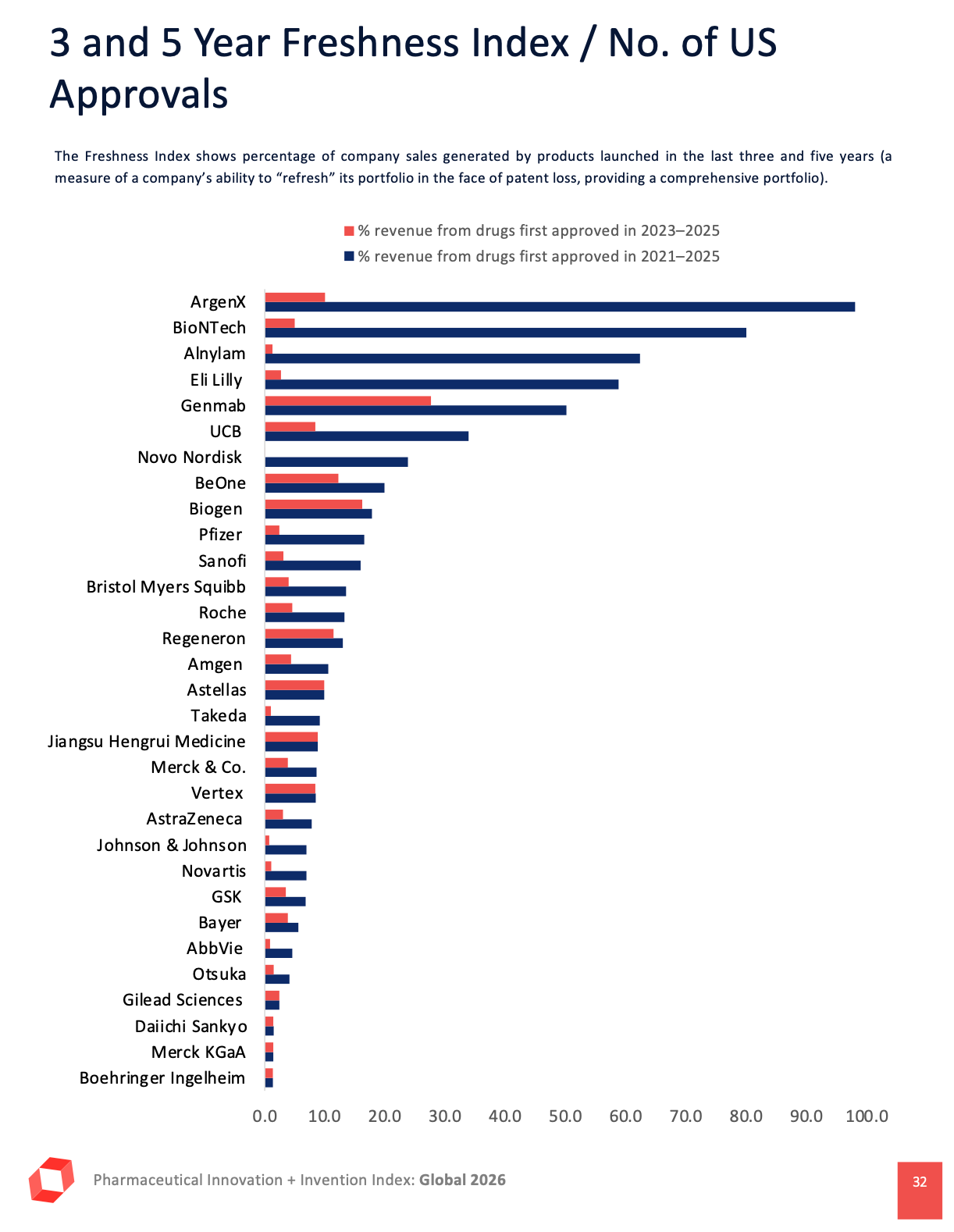
Here’s the Freshness/ Fragility index from IDEA’s report - it’s fair that it focused on US approvals, as many companies are now questioning whether global (mostly EU) launches make sense; no-one questions that they’ll launch in the US first.
So… Have I Failed?
Fifteen years of banging this drum and the Princess Bride/ William Goldman meme is still painfully relevant. Maybe I have, a little.
But I remain optimistic. The 2026 Index shows that the gap can be closed. The tools are better. The pressure from investors and patients is higher. And a handful of companies are quietly proving it can be done differently.
The question for all of us in 2026 isn’t whether we can invent more stuff. It’s whether we’re willing to stop performing and start innovating - turning those inventions into medicines that actually reach patients and create lasting value.
Because if we keep using that word the way we have been… well, you know the rest.
Since you’re referencing William Goldman Mike, I like his most famous quote-“nobody knows anything!”