
How Early-Phase Optionality Is Reshaping Biotech ROI

A few years back, in one of my early attempts to pin down what asymmetric learning actually looks like in practice, I wrote that the winners in pharma aren’t the ones who predict the future perfectly (no-one can do that) - they’re the ones who learn asymmetrically: faster, cheaper, and with outsized upside when the data cooperates.
(See the guide I finally got around to writing: Asymmetric learning: what, why, when....)
Phase 1 has always been the foggy morning of drug development - biology more art than science, data points sparse and noisy. But lately, there’s been an active shift. Companies are turning those early phases into high-resolution option-generation engines, using biomarkers, predictive analytics, and adaptive designs to create real optionality: test multiple paths in parallel, enrich the right patients, drop losers fast, expand winners, pivot indications - all before the Phase 3 cash bonfire. This isn’t just efficiency; it’s designed-in competitive advantage. It echoes the “planned serendipity” I’ve explored here (and on LinkedIn before that): deliberately engineering systems that let you recognize and capture value in the unexpected, rather than hoping luck strikes. Early-phase optionality is planned serendipity at scale - small, cheap bets that reveal big asymmetries.
Take Lantern Pharma as a recent standout. In their Phase 1a dose-escalation of LP-184 (a DNA-damaging prodrug in tough, pre-treated solids), they didn’t just collect safety data. Their RADR® AI platform mined the (very noisy) signals and flagged PTGR1 overexpression plus DDR deficiencies (HRD, BRCA mutants, etc.) as predictive for response. The result? 54% disease control in the enriched subset, durable benefits in some. Instead of a broad Phase 2 fishing expedition, they’re now running multiple parallel biomarker-guided arms: PTGR1-high TNBC ± PARP, DDR-deficient NSCLC, recurrent GBM with spironolactone, urothelial. One protocol, multiple targeted bets, early signals to prioritize (or kill) before big commitments. They’ve already gained Orphan and Fast Track designations. This is asymmetric learning in action: AI turns Phase 1 indigestion into precise expansion options. It reminds me of the point I made in A Better Decision Process for Pharma - evaluate 100 options per asset early with better tools, and suddenly you’re not guessing.

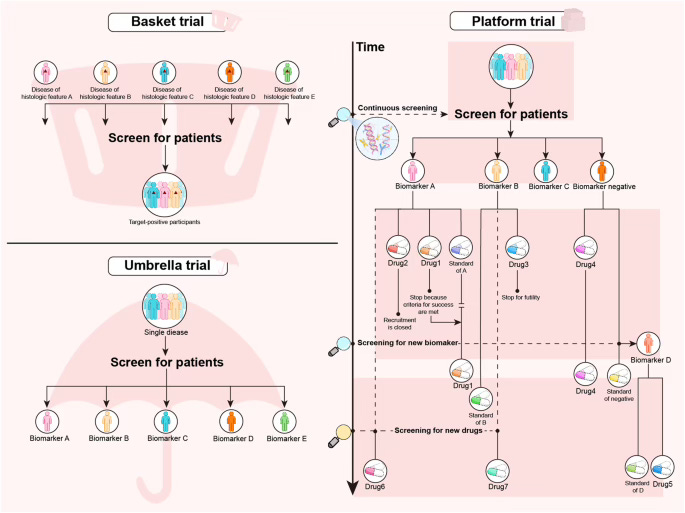
Then there’s AstraZeneca leaning into master/platform protocols. Their ongoing ovarian cancer master (NCT07060365) runs multiple substudies under one umbrella - PARP1-selective agents like saruparib, mono or combo, with upfront biomarker enrichment (e.g., tumor BRCA required for one arm). Single screening, stratified entry, flexible add/drop arms based on emerging data. This is big pharma borrowing from venture thinking: screen once, explore multiple branches simultaneously, use early PoC in subgroups to decide what lives or dies - well before registrational risk. It’s the opposite of the old “one asset, one path” trap. It ties straight into the decision frameworks I’ve been discussing lately (RAVE, DICE, Lilly’s truth-seeking machine) - the best ones reward small, informed bets that compound into advantage.
And outside oncology, Mursla Bio partnering with a big metabolic player on MASH. They isolate hepatocyte-specific EVs from blood (non-invasive, repeatable), generate high-dimensional profiles, feed into AI for MoA maps and responder signatures. This happens pre- or early clinical - enriching inclusion, de-risking targets, informing go/no-go - without biopsies. Liquid biopsy + AI making precision feasible in fibrotic disease, where biomarkers have historically been weak. Again, early human biology data becomes predictive optionality.
These aren’t isolated; they build on trends like adaptive enrichment (enroll broad, restrict to signal-positive at interim) and even digital biomarkers (Roche’s PASADENA Parkinson’s app capturing subtle motor changes classical scales miss). The through-line? Early phase isn’t just dose/safety anymore - it’s where you generate the options that reshape ROI.
Why does this matter for biotech ROI? Because the old model burned cash on all-comers Phase 2/3 hoping for broad efficacy; attrition stayed brutal. Now, winners compress timelines, lower burn, secure designations faster, and create asymmetric upside - small early wins that turn into big later payoffs (or cheap kills). It’s winning small = winning big, as I’ve said before. (Whereas the opposite, ‘losing small’ means ‘not losing big’.)
This shift also forces cultural change - the agility and incentives I’ve harped on since the R&D productivity days. Tech (AI, biomarkers) is the ally, not the savior; the fulcrum is still how teams learn and decide.
As I look back over five years of this newsletter (that retrospective post still feels raw), the thread is consistent: design advantage in, don’t predict it. Early-phase optionality is one of the clearest ways pharma/biotech is finally doing that.